
The Latissimus Dorsi Flap
Written & Edited by Mike Boctor | Filmed on iPhone by Grace McDonnell
Michael J. Boctor, BS, Grace McDonnell, Simon Moradian, MD, Julian Klosowiak, MD, PhD, Jason H. Ko, MD, MBA
The latissimus dorsi flap has been an extraordinary workhorse in reconstructive surgery for over two decades. Situated within the subscapular system, its large vessel diameter and length make it an incredibly versatile and reliable flap. Elevated as a muscle, musculocutaneous, or an osteocutaneous flap, its size can reach up to 20x30cm, making it one of the largest flaps in the body. Adding to its arsenal, it can be tailored to any size or shape, with numerous combinations of flaps nourished by the subscapular system, creating a plethora of possibilities for coverage of complex defects. In addition to providing soft tissue and structural support, it can be used to restore function through a pedicled functional transfer, facilitating movements like elbow flexion, extension, or shoulder abduction. In spite of its size, no significant donor functional deficit results from removal of the muscle… of course with some exceptions
ANATOMY
Anatomic Landmarks
Origin: Mid-point of iliac crest, posterior mid-axial line
Insertion: Lesser tubercle of humerus (anterior to teres major)
Blood Supply
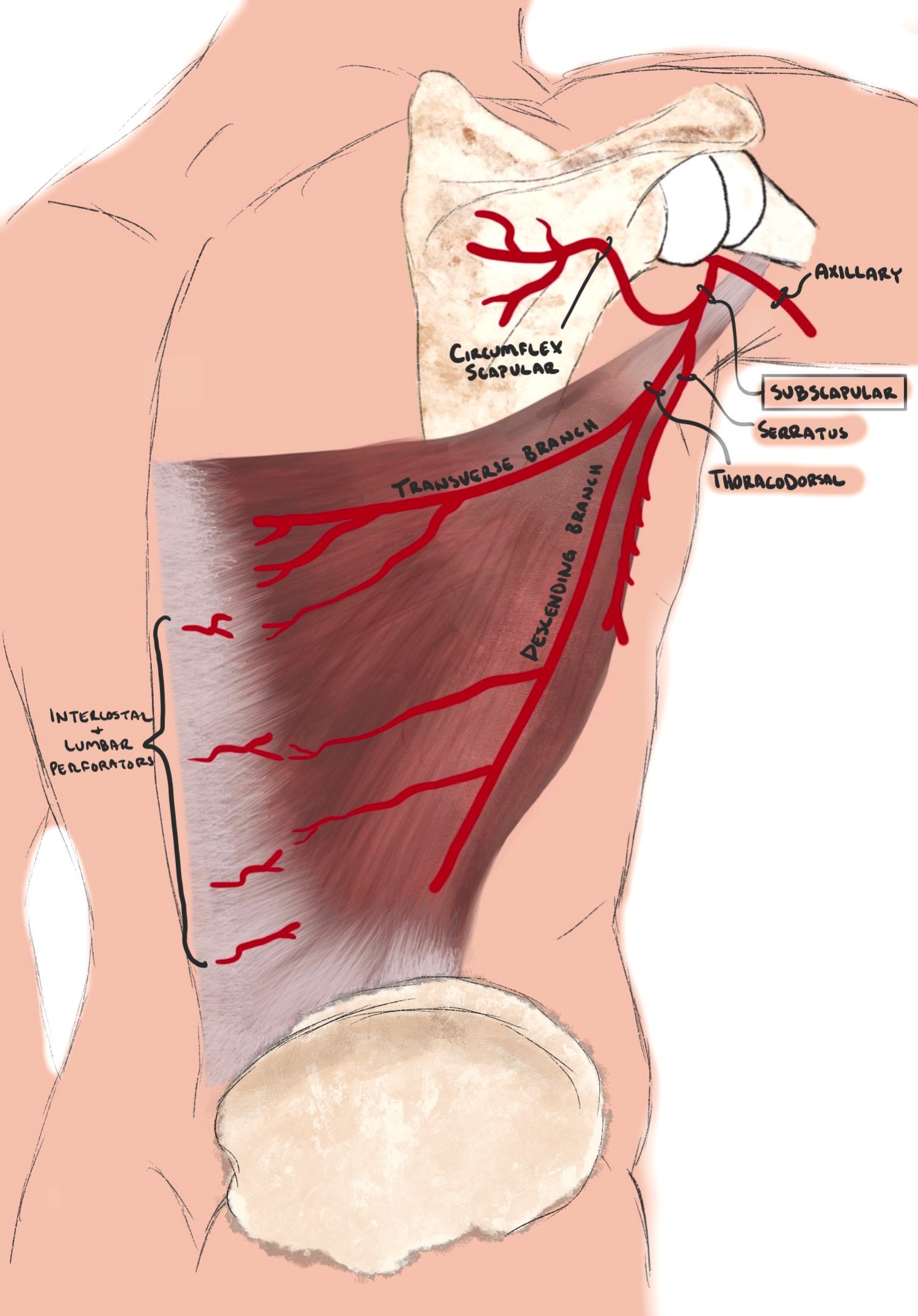
The Latissimus falls under the Type V Mathes-Nahai classification, with a dominant blood supply from the thoracodorsal artery, and segmental circulation from perforators of the posterior intercostal and lumbar arteries. With a large diameter, ranging from 2-5mm, and minimal anatomic variation, the thoracodorsal artery provides a highly reliable blood supply. To review the anatomy of this arterial system, the subscapular artery—which is a branch of the axillary artery—bifurcates to give the circumflex scapular artery, a branch to the serratus, and the thoracodorsal artery. The artery courses the axilla along the anterior border of the muscle, and enters the muscle from the underside. At this point, it spreads into two or three major branches. In more than 90% of cases, it bifurcates into the transverse and descending branches. Both branches run medially, forming large diameter anastomoses with intercostal and lumbar perforators. In addition, numerous musculocutaneous perforators allow for skin island design anywhere on the muscle.
Flap Design
There are a number of ways to design a flap based off of the subscapular system. Based on the thoracodorsal artery alone, the latissimus can be harvested as a pure muscle flap, a musculocutaneous flap, an osteomusculocutaneous flap, or even a pure perforator flap (known as a thoracodorsal artery perforator flap). Many different combinations of skin islands and muscle size are able to be achieved depending on the defect needed to be covered. The diversity of options doesn’t stop there, however, as the subscapular arterial tree creates a vast potential for any combination of chimeric flaps, all of which can be based on a single vascular pedicle.
Chimeric Flaps of Subscapular tree

